Minimally invasive lumbar fusion surgery is an advanced technique designed to treat various lumbar spine conditions such as degenerative disc disease, herniated discs, spondylolisthesis, and spinal deformities. By utilizing smaller incisions and less tissue disruption, this approach offers numerous advantages over traditional open surgery, including faster recovery times, less postoperative pain, and fewer complications.
How Common It Is and Who Gets It? (Epidemiology)
Lumbar spine conditions are prevalent, particularly in older adults, with lumbar disc disease and spinal stenosis being common reasons for lumbar fusion surgery. As individuals age, degenerative changes in the spine, such as the breakdown of intervertebral discs and formation of bone spurs, increase the likelihood of conditions that may require lumbar fusion. Studies suggest that more than 10 million people in the United States suffer from some form of degenerative spine condition, many of whom may be candidates for fusion surgery.
Why It Happens – Causes (Etiology and Pathophysiology)
Conditions treated with lumbar fusion surgery include:
- Degenerative Disc Disease: As discs in the spine lose their elasticity and height, they can cause instability, pain, and nerve compression.
- Spondylolisthesis: The forward slippage of one vertebra over another can lead to instability and compression of spinal nerves.
- Herniated Discs: Discs that bulge or rupture can press on spinal nerves, causing pain, numbness, or weakness in the lower back and legs.
- Spinal Stenosis: Narrowing of the spinal canal that puts pressure on the spinal cord and nerves.
How the Body Part Normally Works? (Relevant Anatomy)
The lumbar spine consists of five vertebrae (L1-L5) and intervertebral discs that cushion the vertebrae, allowing movement and flexibility. The spinal cord runs through the spinal canal, and nerves branch out from the spinal cord to the legs, feet, and other parts of the body. The lamina forms the roof of the spinal canal, and the facet joints provide stability while allowing for spinal movement. Conditions such as disc degeneration or herniation can disrupt this normal function, leading to pain and potential nerve damage.
What You Might Feel – Symptoms (Clinical Presentation)
Symptoms of lumbar spine conditions that may require fusion surgery include:
- Chronic low back pain that doesn’t respond to conservative treatments.
- Radiating leg pain (sciatica) due to nerve compression.
- Numbness, tingling, or weakness in the legs and feet.
- Difficulty walking or maintaining balance, especially when bending backward or walking downhill.
How Doctors Find the Problem? (Diagnosis and Imaging)
Diagnosis typically involves:
- Physical Examination: To assess muscle strength, reflexes, and pain levels.
- MRI and CT Scans: To visualize spinal alignment, disc degeneration, herniated discs, or narrowing of the spinal canal.
- X-rays: To identify bone spurs, fractures, or signs of instability.
- Electromyography (EMG): To assess nerve function and determine if there is nerve compression.
Classification
Lumbar fusion can be classified based on the surgical approach:
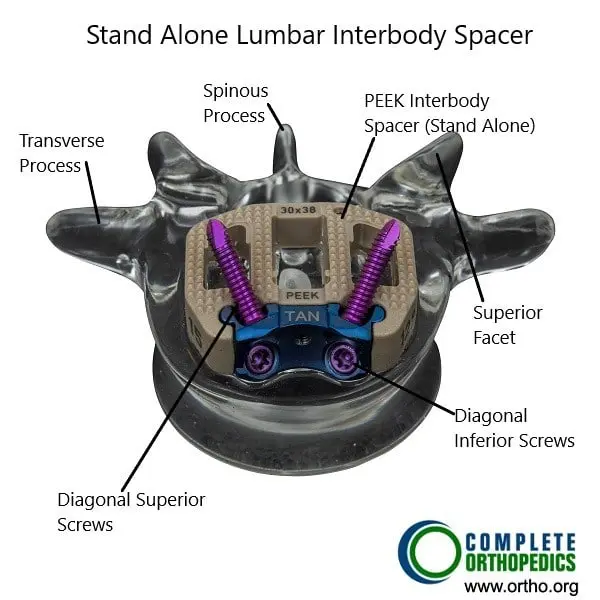
- Anterior Lumbar Interbody Fusion (ALIF): Performed from the front of the spine.
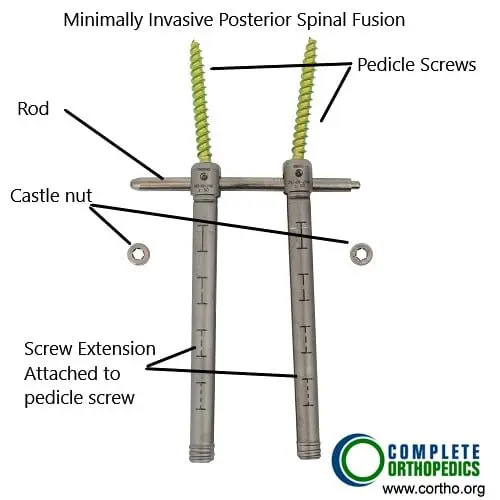
- Posterior Lumbar Interbody Fusion (PLIF): Performed from the back.
- Transforaminal Lumbar Interbody Fusion (TLIF): Performed through a small incision in the back at an angle.
- Posterolateral Fusion: Involves fusing the sides of the vertebrae without removing the disc.
Other Problems That Can Feel Similar (Differential Diagnosis)
Conditions that can mimic lumbar spine problems include:
- Piriformis Syndrome: Pressure on the sciatic nerve by the piriformis muscle.
- Hip Arthritis: Can cause pain that radiates to the lower back or buttocks.
- Muscle Strains: Often mistaken for spinal problems due to similar pain patterns.
- Kidney Stones: Can cause pain in the lower back that may mimic spinal issues.
Treatment Options
Non-Surgical Care
- Physical Therapy: Strengthening exercises to stabilize the spine.
- Medications: NSAIDs or corticosteroids to reduce inflammation and pain.
- Epidural Steroid Injections: For relieving inflammation around spinal nerves.
Surgical Care
- Minimally Invasive Lumbar Fusion: The primary surgical option, which involves fusing two or more vertebrae using smaller incisions and specialized instruments.
- Traditional Lumbar Fusion: Involves a larger incision and more extensive tissue dissection.
- Minimally Invasive Techniques for ALIF, PLIF, and TLIF: These techniques use small incisions and minimize muscle dissection.
Recovery and What to Expect After Treatment
Postoperative care typically includes:
- Pain Management: Controlled with medications, and physical therapy to improve strength and flexibility.
- Hospital Stay: Patients often go home the same day or after a short stay, depending on the procedure.
- Physical Therapy: To aid in recovery, restore mobility, and reduce the risk of complications.
- Activity Restrictions: Avoid heavy lifting or high-impact activities during recovery.
Possible Risks or Side Effects (Complications)
Potential complications include:
- Infection: At the surgical site.
- Blood Clots: Increased risk of deep vein thrombosis (DVT).
- Nerve Injury: Although rare, there is a risk of nerve damage during surgery.
- Implant Failure: In the case of hardware used to stabilize the spine.
- Failed Fusion: When the vertebrae do not properly fuse.
Long-Term Outlook (Prognosis)
The prognosis for minimally invasive lumbar fusion is generally excellent, with most patients experiencing significant pain relief and improved function. However, long-term outcomes depend on factors such as the patient’s overall health, the specific spinal condition, and adherence to postoperative care.
Benefits of Minimally Invasive Lumbar Surgery
Reduced Tissue Damage and Postoperative Pain
One of the primary advantages of MIS is the reduced damage to muscles and soft tissues. Smaller incisions and less muscle dissection result in decreased postoperative pain and a quicker return to normal activities. Patients undergoing MIS often experience less postoperative discomfort and require fewer pain medications compared to those undergoing traditional open surgery.
Shorter Hospital Stays and Faster Recovery
MIS techniques are associated with shorter hospital stays and faster recovery times. Many MIS procedures can be performed on an outpatient basis or with a brief hospital stay. The reduced trauma to tissues and lower risk of complications contribute to a quicker recovery, allowing patients to resume their daily activities sooner. The articles reviewed highlight the positive impact of MIS on postoperative recovery, with many patients returning to work and normal life within a few weeks of surgery.
Lower Risk of Complications
The minimally invasive nature of these procedures reduces the risk of complications such as infection, blood loss, and muscle atrophy. The smaller incisions and precise instrumentation used in MIS minimize the exposure of internal tissues to potential contaminants, decreasing the likelihood of postoperative infections. Additionally, the reduced need for blood transfusions and the preservation of muscle function contribute to better overall outcomes for patients.
Improved Cosmetic Outcomes
Smaller incisions and reduced scarring are significant cosmetic benefits of MIS. Patients often appreciate the improved aesthetic outcomes, which can contribute to higher satisfaction with the surgical procedure. The articles underscore the importance of these cosmetic benefits, especially for younger patients and those concerned about the appearance of their surgical scars.
Out-of-Pocket Costs
Medicare
CPT Code 22558 – Anterior Lumbar Interbody Fusion (ALIF) / Lateral Lumbar Interbody Fusion (LLIF): $368.50
CPT Code 22630 – Posterior Lumbar Interbody Fusion (PLIF) / Transforaminal Lumbar Interbody Fusion (TLIF): $387.42
CPT Code 22612 – Posterior Lumbar Fusion (PLF): $382.85
Under Medicare, 80% of the approved cost for these procedures is covered once your annual deductible has been met. The remaining 20% is typically the patient’s responsibility. Supplemental insurance plans—such as Medigap, AARP, or Blue Cross Blue Shield—generally cover this 20%, leaving most patients with little to no out-of-pocket expenses for Medicare-approved lumbar fusion surgeries. These supplemental plans coordinate directly with Medicare to ensure full coverage for these complex spine surgeries.
If you have secondary insurance—such as Employer-Based coverage, TRICARE, or Veterans Health Administration (VHA)—it serves as a secondary payer once Medicare has processed the claim. After your deductible is satisfied, the secondary plan may cover any remaining balance, including coinsurance or small residual charges. Secondary plans typically have a modest deductible, usually between $100 and $300, depending on your specific policy and network status.
Workers’ Compensation
If your lumbar spine condition requiring fusion surgery is work-related, Workers’ Compensation will fully cover all treatment-related costs, including surgery, instrumentation, and rehabilitation. You will have no out-of-pocket expenses under an accepted Workers’ Compensation claim.
No-Fault Insurance
If your lumbar spine injury resulting in fusion surgery is caused by a motor vehicle accident, No-Fault Insurance will pay for all medical and surgical expenses, including ALIF, LLIF, PLIF, TLIF, and posterior lumbar fusion. The only potential out-of-pocket cost may be a small deductible depending on your policy terms.
Example
Paul, a 64-year-old patient with lumbar disc degeneration and nerve compression, required anterior lumbar interbody fusion (CPT 22558) and posterior lumbar fusion with instrumentation (CPT 22612). His estimated Medicare out-of-pocket costs were $368.50 for the ALIF and $382.85 for the posterior fusion. Since Paul had supplemental insurance through Blue Cross Blue Shield, the 20% that Medicare did not cover was fully paid, leaving him with no out-of-pocket expenses for his surgery.
Frequently Asked Questions (FAQ)
Q. How long is the recovery after minimally invasive lumbar fusion surgery?
A. Recovery time is typically shorter than traditional open surgery, with most patients returning to normal activities within 6-8 weeks. Full recovery may take several months.
Q. Will I experience less pain with minimally invasive surgery?
A. Yes, patients generally report less postoperative pain compared to traditional open surgeries due to smaller incisions and less tissue disruption.
Q. Is minimally invasive lumbar fusion suitable for everyone?
A. While it offers many advantages, not all patients are candidates for minimally invasive surgery. Your surgeon will assess your condition to determine the best approach.
Summary and Takeaway
Minimally invasive lumbar fusion surgery is an advanced, less traumatic alternative to traditional open surgery for treating lumbar spine conditions. With smaller incisions and reduced tissue disruption, patients experience quicker recovery, less pain, and fewer complications. However, not all patients are candidates for this procedure, and a thorough evaluation by a skilled surgeon is crucial to determine the most appropriate treatment.
Clinical Insight & Recent Findings
A recent study compared three types of minimally invasive lumbar fusion techniques—MIS-TLIF, OLIF, and Endo-TLIF—for the treatment of L4/L5 degenerative spondylolisthesis, revealing significant advantages of the OLIF approach.
Patients undergoing OLIF experienced less blood loss, shorter hospital stays, and lower drainage volumes compared to those receiving MIS-TLIF or Endo-TLIF. Additionally, the OLIF group showed superior outcomes in maintaining lumbar lordosis angle (LLA) and disc height (DH), contributing to better functional outcomes, particularly for back pain.
The study highlights OLIF’s benefits, including better preservation of posterior spinal structures and a higher fusion rate, making it a preferred option for L4/L5 spondylolisthesis. (“Study on minimally invasive lumbar fusion techniques for spondylolisthesis – see PubMed“)
Who Performs This Treatment? (Specialists and Team Involved)
Minimally invasive lumbar fusion is performed by:
- Spine Surgeons: Specializing in lumbar spine conditions.
- Anesthesiologists: Managing anesthesia during surgery.
- Physical Therapists: Assisting in postoperative rehabilitation.
When to See a Specialist?
If you experience persistent or worsening back pain, leg pain, numbness, or weakness despite conservative treatment, it may be time to consult a spine specialist to discuss the possibility of lumbar fusion surgery.
When to Go to the Emergency Room?
Seek emergency care if you experience:
- Sudden loss of bladder or bowel control.
- Severe, unrelenting pain.
- Sudden weakness or numbness in the legs.
What Recovery Really Looks Like?
Patients typically experience a faster recovery with minimally invasive lumbar fusion compared to traditional surgery. Most can return to light activities within weeks, though full recovery may take several months.
What Happens If You Ignore It?
Ignoring symptoms of spinal instability or nerve compression can lead to worsening pain, permanent nerve damage, and a decrease in mobility. Early intervention with surgery often results in better outcomes.
How to Prevent It?
Maintaining a healthy weight, practicing good posture, and engaging in regular exercise to strengthen the back muscles can help prevent lumbar spine issues.
Nutrition and Bone or Joint Health
A balanced diet with adequate calcium, vitamin D, and protein supports bone healing and overall spine health. Staying hydrated and avoiding smoking also help recovery.
Activity and Lifestyle Modifications
Gradual return to activity, proper body mechanics, safe lifting habits, and ongoing strengthening exercises help protect the spine long term. Regular low-impact activity such as walking or swimming supports continued health.
¿Tienes más preguntas?
How do I schedule a consultation with an orthopedic surgeon at Complete Orthopedics?
Consultations can be scheduled online through the Complete Orthopedics website or by calling their office directly.
When can I go back to work after minimal invasive back surgery?
Patients with minimal invasive back surgery have an earlier recovery than patients who undergo open surgeries. These patients can get back to desk-type job within two to three weeks. Patients who are in high demand job may take up to eight to twelve weeks to get back to their normal job, which includes work or sports. Physical therapy and rehabilitation may have a role to play in recovery of these patients.
How soon after the surgery can I start physical therapy?
Patients are not required to start their physical therapy till two weeks after the surgery. After two weeks of surgery, physician reexamination will help in deciding if the patient requires physical therapy or not. Many of the patients do not require physical therapy after the surgery.
Does smoking cause spine problems?
Smoking has proven to cause spine problems, including neck and lower back. At the same time, smoking is detrimental for patients who require spine surgery, especially fusion surgeries. It has been shown that smoking delays spine fusion, as well as lead to higher incidence of nonunion and possible need for revision surgeries
What if, during my surgery, you encounter a different issue other than expected?
Usually, before the surgery, we discuss with the patient regarding all the possible spine issues that we may expect and how to manage them. If there is an unexpected issue, which has not been discussed earlier, we would go ahead and discuss it with the patient’s relative and treat it accordingly from there. If there is something which can wait, and is not detrimental to the patient, and relatives are not able to make decision on it, we may leave it for a later date to be discussed with the patient after the surgery.
How long is it possible to stay for back surgery?
Most of the patients with back surgery can be discharged within one to four days after the surgery depending on the type of surgery and the type of recovery that they have. Patients who undergo complex spine surgeries may need longer period of hospitalization and recovery.
Which pain medications will I be sent home with? What are the possible side-effects of these prescriptions?
Most of the patients with cervical spine surgery, will be sent with some narcotic pain medication to take care of their pain. These medications do have their multiple side-effects, which may be constipation, nausea, vomiting, impaired judgement, drowsiness, headache. Though patients who are treated with narcotic pain medication for acute pain, mostly do not lead to addiction, but these medications do have addiction potential.
Will you know before the surgery if I need a brace afterwards? If so, will I be fitted for one before the surgery?
Most of the patients with spine surgery do not need a brace. If we expect that the patient will need a brace, we will get the patient pre-fitted with a brace so that it is available immediately after the surgery. Occasionally the need for brace may be decided at the time of surgery. In such cases a brace is arranged in immediate post-operative period.
Will I need any other medical equipment like a walker when I go home? Should I get an adjusted bed or sleep downstairs?
Patient may need other medical equipment like walker or a stick. If that is required, patients are provided with such equipment in the hospital before their discharge and are trained how to use them by the physical therapist and occupational therapist. If the patient needs to use stairs, patients are trained by the physical therapist before they are let go home. If the patient needs an adjustable bed, they are informed about that. That can be done prior to the surgery. It is desirable for patients to stay downstairs for a few weeks if possible.
Who can I call if I have questions after the surgery?
In case patient has routine questions regarding after the surgery or regarding the surgery, they can call the physician’s office and talk to the nurse or secretary or the physician. If they’re not available on the phone, they can leave a voice mail and they will be answered later. In case the patient has a medical emergency, then they should not call the physician office but rather call 911 or get to the hospital ER as soon as possible.
How often will I see you after my surgery?
Patients are usually followed at two weeks, six weeks, three months, six months, and a year after surgery.
What symptoms would warrant a call to your office after the surgery?
If the patient develops problems like chest pain, breathing problems, sudden neurological deterioration, or any other emergency they should call 911, or go to the emergency room directly. Patients who develop worsening pain at the surgery site, discharge from the wound, fever; they should call in the office.
How long should I wait to bathe after the surgery?
Patients are usually asked to avoid bathing, until the incision heals, which may take two to three weeks. Patient can take shower after 72 hours of surgery with an impervious dressing in place. The dressing can be changes if the wound is visibly soaked. Patients are asked not to rub the area of surgery for about two to three weeks. They can gently dab it dry with a towel.
How long will I be out of work?
Patients with low demand work and desk job, can be back to work as soon as three to six weeks after the surgery depending on patient pain control as well as recovery. Patients who are in heavy lifting or control of heavy machinery or handyman job, may take three to four months, or even more to get back to work depending on their recovery from the surgery.
How soon after the surgery can I start physical therapy?
Patients after back surgery are usually started on physical therapy, if they need, depending on physician’s advice, at two to four weeks after the surgery. Many of the patients do not need physical therapy. A decision to go into physical therapy will depend on the surgery as well their recovery.
What if I get an infection?
If the patient has a superficial infection, few days of antibiotics will help heal these infections. Occasionally patient may develop deep infection. In these patients may need IV antibiotics for a longer period. If despite all efforts or in patients with rapid deterioration due to infection, surgery may be needed to help clean off the infection.
How common is surgery?
Most of the patients do not need surgery and can be treated with conservative means. When the patients do not respond to conservative measures, or if they have worsening neurological deficit, or worse pain, they may need surgery.
Will I have irreversible damage if I delay surgery?
Patients who develop neurological deficit in the form of weakness or involvement of bowel or bladder may have irreversible damage if the surgery is delayed enough.
When do I need fusion?
When patient has back pain or has a surgery in which enough bone is removed to destabilize the spine, in these cases patient may need a fusion surgery to stabilize the spine, as well as to alleviate the symptoms. What are my risks of low back surgery?
When will I be back to my normal activities?
Though these things depend on the type of surgery patient has undergone, patient can usually be progressively back to their normal activities, starting from three to five days from surgery. Patients are encouraged to take care of their activities of daily living, as well as light household activities. Patients can get back to driving once they are free from pain medication and are able to sit for a duration of period for driving, which may take upto 2-3 weeks or more.
What type of surgery is recommended? The type of surgery depends on the presenting complaint, examination findings, as well as imaging findings in the form of x-ray and MRI. Some patients may need to undergo just discectomy, or laminectomy, while others may need a fusion surgery on their back to relieve their symptoms. To know more about the type of surgery, the patient needs to discuss this with their spine surgeons.
What type of surgery is recommended? The type of surgery depends on the presenting complaint, examination findings, as well as imaging findings in the form of x-ray and MRI. Some patients may need to undergo just discectomy, or laminectomy, while others may need a fusion surgery on their back to relieve their symptoms. To know more about the type of surgery, the patient needs to discuss this with their spine surgeons.
How long will the surgery take?
Spine surgeries like discectomy and laminectomy usually last about one to one and a half hours. Spine fusion surgeries, may take longer periods, up to two and a half to four hours or more. It depends on type of surgery, and as well as the level of spine to be operated upon.
What is degenerative disc disease?
Degeneration means gradual damage of the tissue. Degenerative disc disease represents aging of the disc, either appropriate to the normal age of the patient, or maybe accelerated due to injury or chronic disease, or other factors like smoking, obesity.
What is Lumbar instability?
Lumbar instability means that the spine is not stable and there is excessive abnormal movement between two vertebrae. This is usually diagnosed by imaging in the form of X-rays, CT scan, or MRI of the patients. Instability may lead to compression of nerve roots causing radiculopathy with or without back pain.
What is sciatica?
Sciatica is another name for lumbar radiculopathy, in which patient has pain going down their legs. The pattern of pain depends on the nerve root involved, but the most common is pain going down the outer side of the thigh and leg into the foot.
What is spinal stenosis?
Spinal Stenosis means narrowing of the spinal canal. It is can be at the cervical or thoracic or lumbar level. Most common spinal stenosis is at lumbar level and it, when narrowed, can compress nerves, causing pain going down the legs, with or without tingling, numbness, weakness, or involvement of bowel or bladder.
What is lumbar disc disease? how is this problem diagnosed?
The diagnosis of Lumbar disc disease is made by history and examination of the patient. The confirmation of diagnosis is done by imaging in the form of X-rays and MRI. Occasionally the patient is having contraindication to MRI, patient may need to undergo a CT scan. When a CT scan is done, occasionally the patient may need to get injected with a dye before the CT scan and this is called CT myelography. Occasionally patient may need a CT scan along with MRI also.
When should I consider surgery for the back pain?
Most of the patients get treated with conservative means. In case the patient is not getting relief despite continuous conservative measures, or if there is worsening of pain associated with or without weakness or involvement of bowel or bladder, the patient may need surgical intervention in the form of surgery.
Am I a candidate for minimal-invasive spine surgery?
Some patients are good candidates for minimally-invasive spine surgery and they can get better with that. History, physical examination, as well as special investigations like X-ray and MRI, are needed in order to discuss regarding options of minimal invasive spine surgery. Some patients are not good candidates for minimal invasive spine surgery and doing such a surgery in such patients may lead to non-resolved solution of the symptoms or worsening.
Will I need physical therapy after I get minimally-invasive spine surgery?
Many patients may require physical therapy after spine surgery, including minimally-invasive spine surgery. The decision to go for physical therapy is taken by the spine surgeon and depends on the condition of the patient, as well as the surgery done. Physical therapy may be required for optimal rehabilitation and recovery of strength of the muscles.
What is a minimal invasive TLIF?
TLIF is a usual form of fusion surgery that is done in lower lumbar spine from the back, in which a cage is put between the vertebral bodies, along with screws to enhance the potential body fusion. Minimally-invasive TLIF means to do the surgery through minimally-invasive methods, in which there are multiple small incisions through which the surgery is done. The surgery in such a case has decreased blood loss and early recovery.
Are there any warning symptoms?
Warning symptoms of lumbar disc disease include worsening pain, tingling and numbness, development of weakness, or worsening of weakness, involvement of bowel or bladder in the form of incontinence of urine or stools, presence of fever, unintentional weight loss. In such conditions patients should immediately seek medical attention.
Do you need any tests?
General blood workup is needed in most patients before the surgery. This will include blood counts as well as metabolic profile. Special tests may be needed in some patients if the physician has suspicion of some other disease. Most of the patients will have to undergo X-ray and MRI, or a CT scan before the surgery to confirm their diagnosis.
What are the possible surgical complications from a low back surgery?
Common complications of a low back spine surgery are bleeding, infection, leak of cerebral spinal fluid temporary or permanent neurological deficits, blindness, worsening of pain, failure of fusion, failure of implants. There may be risks due to the anesthesia also.
