Overview
Sciatica involves symptoms of low back pain radiating down the leg that may occur on one side or both sides. The most common cause of sciatica or lumbar radiculopathy is intervertebral disc herniation. The sciatica symptoms may affect pregnant females more so during the 2nd and the 3rd trimester of pregnancy.
Pregnancy-related sciatica usually responds to conservative management. Although back pain is a common complaint during pregnancy, sciatica-related back pain is rare in pregnant females.
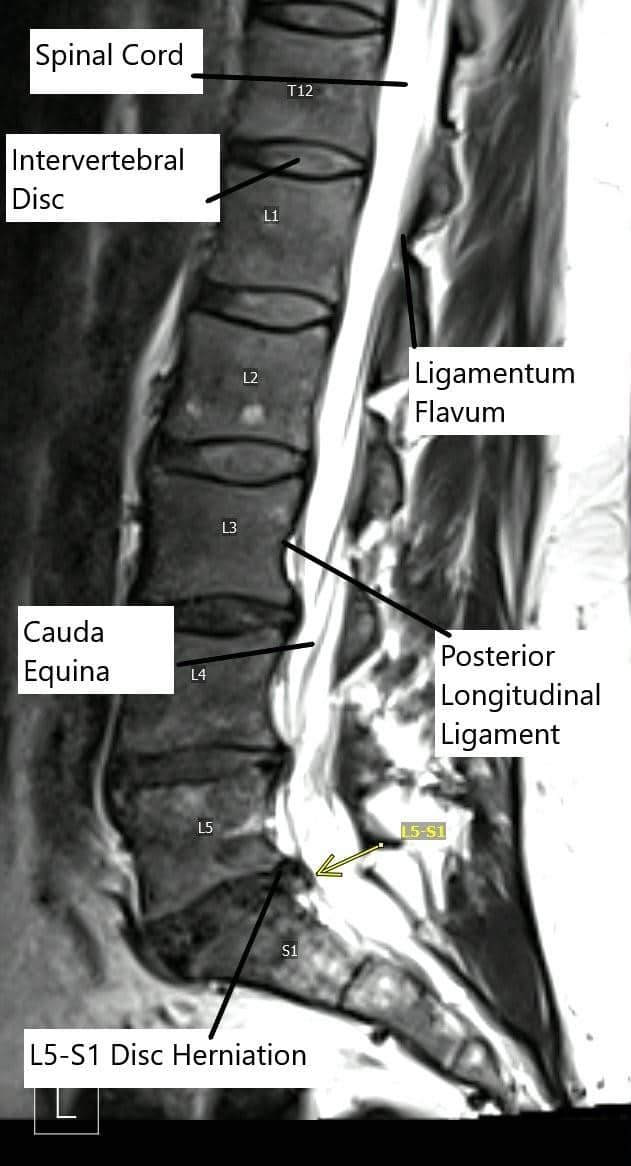
Sagittal section of the lumbar MRI showing L5-S1 disc herniation.
The sciatic nerve is a large nerve originating near the lower spine and travels down the pelvis to enter the back of the thigh. The nerve supplies the major muscles in the thigh, legs, and feet. The nerve is also responsible for transmitting the sensory signals from the feet, legs, and the back of the thigh.
The nerve roots (L4, L5, S1, S2, and S3) exit the neural foramen at different levels and join together to form the sciatic nerve. Any compression or narrowing of the space available for the nerves may lead to the symptoms of sciatica.
A prolapsed intervertebral disc is a common culprit as the herniated disc may impinge upon the exiting or traversing nerve roots. A prior disc bulge or herniation may get exacerbated during pregnancy. Pregnancy is associated with weight gain which may add to the increased pressure on the intervertebral disc.
The center of gravity of the body changes as the abdominal girth increases, the body tries to align the center of gravity by increasing the backward curve of the lower spine and tilting the pelvis forward. This may increase the amount of force acting on the intervertebral discs and discs may herniate.
During pregnancy, a hormone known as relaxin is released especially during the end trimester. The relaxin hormone aids to relax the ligaments and joints of the pelvis for the smooth delivery of the baby. There may be an association of relaxation of the ligaments in the spine that may lead to herniation of the intervertebral disc.
Back pain is a common symptom in pregnancy that is mostly unrelated to sciatica but a physician’s examination may be necessary to differentiate different causes of the back pain. Pregnant females may complain of pain in the buttock/lower back that may radiate down to the leg or the toes. The pain may be associated with a feeling of burning or tingling.
In some cases due to significant compression of the nerve roots, there may be symptoms of weakness and numbness in the legs. Rarely, patients may complain of bowel or bladder incontinence.
The physician may examine and conduct a physical examination to localize the cause of symptoms. The physical examination may include tests to check the power and sensory integrity of the spine in the lower extremities. Almost all cases of sciatica are diagnosed clinically and do not require imaging.
Sciatica in pregnancy is managed with conservative methods. The patients are encouraged to continue staying active and avoid activities that exacerbate the symptoms. Conservative management consists of the use of pregnancy-safe pain relief medications such as Tylenol. Medications such as nonsteroidal anti-inflammatory medication like ibuprofen are avoided in pregnancy.
Patients are often advised to modify their activities and their sleeping positions to achieve relief. Physical therapy is recommended to improve flexibility and strengthen the muscles around the back. Exercises in pregnancy are only recommended only under the observation of a trained therapist.
Cold therapy may be used in patients with sudden onset of sciatica. Cold therapy works by numbing the nerves responsible for transmitting the pain signals and reducing the blood flow to the affected segment. The reduced blood supply decreases the number of inflammatory cells reaching the area, thus reducing pain and swelling. The cold therapy may be given by applying ice packs to the affected area.
In the case of chronic sciatica, heat therapy may benefit the patients by increasing the blood flow to the affected area. The increased blood flow helps by increasing the number of nutrients reaching the site of inflammation, resulting in quicker recovery. The heat therapy may be done with a warm bottle or a warm heating pad.
The patients who do not benefit from a trial of conservative therapy for 4-5 weeks may benefit from epidural or transforaminal steroid injection. The local injection of the steroid in the affected area reduces the inflammation and provides relief from symptoms. The injection may provide relief for a few months and maybe repeated to extend the relief.
Surgical management is rarely indicated for sciatica in pregnancy. The majority of the pregnant females experience significant relief from sciatica symptoms after the delivery. Surgery may be required immediately in patients in whom there are signs and symptoms of cauda equina syndrome. The symptoms of cauda equina syndrome include loss of bowel/bladder control, numbness of the saddle area, and weakness/numbness of the legs.
Surgery may also be required in patients with worsening symptoms and signs of motor/sensory weakness. The timing, type, and approach of the surgery depend upon the level of nerve root compression and the gestational age of the child. Usually, a microdiscectomy or endoscopic disc removal surgery may be performed. Sometimes, the surgery may be postponed until the birth of the baby.
Conlusion
In conclusion, sciatica during pregnancy, while uncomfortable and potentially disruptive, is generally a manageable condition with appropriate care. Understanding the causes, symptoms, and treatment options can help alleviate anxiety and empower pregnant women to take proactive steps toward relief. Conservative treatments, including physical therapy, modified exercise, and pain management strategies, are usually effective in mitigating symptoms. It’s important for pregnant women experiencing sciatica to seek medical advice early, especially if symptoms are severe or worsening, to ensure the best outcomes for both mother and baby. With careful management and support, most women find significant relief from sciatica symptoms post-pregnancy, allowing them to focus on the joys of motherhood.
Do you have more questions?
Can sciatica in pregnancy harm the baby?
Sciatica itself does not harm the baby. It primarily affects the mother’s comfort and mobility. However, severe pain and discomfort might indirectly impact the mother’s well-being.
What are the safe ways to relieve sciatica pain during pregnancy?
Safe methods include physical therapy, modified exercise routines, cold and heat therapy, proper posture, and Tylenol for pain relief. It is important to avoid NSAIDs like ibuprofen unless specifically advised by a healthcare provider.
How does pregnancy affect existing sciatica?
Pregnancy can exacerbate pre-existing sciatica due to weight gain, shifting center of gravity, and hormonal changes that relax ligaments, potentially leading to disc herniation or increased pressure on the sciatic nerve.
How long does sciatica typically last during pregnancy?
Sciatica during pregnancy often improves after delivery as the pressure on the sciatic nerve decreases. However, the duration can vary depending on the severity of nerve compression and the individual’s response to conservative treatment.
Is it safe to do physical therapy during pregnancy for sciatica?
Yes, physical therapy is often recommended to manage sciatica during pregnancy. Exercises should be tailored by a trained therapist to ensure they are safe for both the mother and baby.
When should a pregnant woman with sciatica see a doctor?
A doctor should be consulted if sciatica symptoms are severe, persistent, or if there is associated weakness, numbness, or bowel/bladder incontinence, which could indicate a more serious condition like cauda equina syndrome.
Can sciatica be prevented during pregnancy?
While sciatica cannot always be prevented, maintaining a healthy weight, practicing good posture, and performing regular exercise under guidance can reduce the risk. Avoiding prolonged sitting or standing can also help.
Are there any exercises pregnant women should avoid if they have sciatica?
Pregnant women with sciatica should avoid high-impact activities, heavy lifting, or any exercise that exacerbates pain. Exercises should be low-impact, focusing on stretching and strengthening the back and pelvic muscles.
What is the role of a chiropractor in treating pregnancy-related sciatica?
A chiropractor may help by performing adjustments to relieve pressure on the sciatic nerve. However, it is crucial to ensure the chiropractor has experience treating pregnant women and that the techniques used are safe during pregnancy.
Can sciatica cause permanent nerve damage if untreated during pregnancy?
While sciatica typically resolves after pregnancy, untreated severe cases can potentially cause prolonged nerve compression, leading to chronic pain or permanent nerve damage, though this is rare.
What sleeping positions are best for relieving sciatica during pregnancy?
Sleeping on the side with a pillow between the knees can help align the spine and reduce pressure on the sciatic nerve. A pregnancy pillow can also provide additional support.
How does the weight gain in pregnancy contribute to sciatica?
Weight gain, especially in the abdomen, shifts the center of gravity and increases the load on the lumbar spine and intervertebral discs, potentially leading to disc herniation and sciatica.
Is swimming safe for pregnant women with sciatica?
Swimming is generally safe and beneficial as it reduces the load on the spine and joints while providing a gentle workout for the back and pelvic muscles. However, any discomfort should be discussed with a healthcare provider.
Can sciatica be confused with other conditions during pregnancy?
Yes, sciatica symptoms can be similar to other conditions like pelvic girdle pain or lumbar strain. A thorough evaluation by a physician is necessary to accurately diagnose and differentiate between these conditions.
Is it possible for sciatica to worsen postpartum?
In some cases, sciatica may persist or worsen postpartum due to ongoing inflammation or strain from labor and delivery. However, most women experience relief as their body returns to pre-pregnancy conditions.
What are the risks of epidural steroid injections for sciatica during pregnancy?
While generally considered safe, there is limited research on the effects of epidural steroid injections during pregnancy. The risks should be weighed against the potential benefits, and such treatments should be done under strict medical supervision.
Can yoga help manage sciatica during pregnancy?
Prenatal yoga, with a focus on gentle stretches and strengthening exercises, can help manage sciatica. It is important to work with a qualified instructor familiar with sciatica and pregnancy to avoid poses that could aggravate the condition.
How does the hormone relaxin contribute to sciatica during pregnancy?
Relaxin softens the ligaments and joints to prepare the body for childbirth, which can also lead to instability in the spine and increased susceptibility to disc herniation, potentially causing sciatica.
What should be avoided during sciatica flare-ups in pregnancy?
Activities that exacerbate symptoms, such as heavy lifting, prolonged sitting, or standing, and improper posture should be avoided during sciatica flare-ups. Rest and gentle movement are key to managing symptoms.
Is there a connection between sciatica and varicose veins in pregnancy?
While sciatica and varicose veins are different conditions, both can be caused by increased pressure on the lower body during pregnancy. Compression from the uterus on veins and nerves may contribute to both issues.
Can sciatica cause complications during labor?
Sciatica usually does not cause complications during labor, but severe pain or nerve compression might impact the mother’s mobility and comfort. Discussing pain management strategies with the healthcare team is essential.
Is massage therapy effective for sciatica during pregnancy?
Prenatal massage therapy can be effective in relieving sciatica symptoms by reducing muscle tension and improving circulation. It should be performed by a therapist trained in prenatal care.
How does childbirth impact sciatica symptoms?
Many women experience significant relief from sciatica after childbirth as the pressure on the sciatic nerve decreases. However, the delivery process can sometimes temporarily worsen symptoms due to physical strain.
Can sciatica lead to permanent disability if untreated during pregnancy?
Permanent disability from sciatica during pregnancy is rare, especially with appropriate management. However, severe and untreated cases can lead to prolonged recovery or chronic pain.
